Vol. 13, n. 3, novembre 2020
STUDI E RICERCHE
Promuovere un invecchiamento in salute
Uno studio sulle determinanti psicologiche dell’adesione alla dieta Mediterranea in età anziana e sue implicazioni per gli interventi
Manuela Zambianchi1
Sommario
Lo studio ha analizzato, attraverso un modello modificato della Teoria del Comportamento Pianificato, il ruolo rivestito dall’adesione passata alla dieta Mediterranea, la credenza che la dieta Mediterranea possa contribuire alla salute nell’età anziana e le strategie proattive di coping sull’intenzione di aumentare la sua aderenza. Hanno preso parte allo studio 121 persone anziane (età media: 68.60 a. DS = 7.1; 63 maschi e 51 femmine, 7 non hanno inserito questi dati demografici), le quali hanno compilato i seguenti strumenti: Questionario sull’aderenza alla dieta Mediterranea (Panagiotakos, Pitsavos, & Stefanidis, 2007); Inventario sul Coping Proattivo (Greenglass, 2002); un single item ha valutato l’intenzione di aumentare l’aderenza alla dieta Mediterranea. Le femmine risultano più intenzionate di aderire alla dieta mediterranea, ed una maggiore scolarità ne favorisce l’aderenza. Un Modello Lineare Generale ha evidenziato il contributo positivo offerto da tre variabili indipendenti: le strategie proattive di coping, la credenza che la dieta mediterranea aiuti le persone anziane a raggiungere un invecchiamento in salute e l’adesione passata ad essa, assieme al genere, il livello di educazione scolastica e all’interazione tra genere e livello di scolarità.
Parole chiave
Dieta Mediterranea, invecchiamento in salute, coping proattivo, Teoria del Comportamento Pianificato.
STUDIES AND RESEARCHES
Promoting a healthy aging
A study on the psychological determinants of adherence to the Mediterranean diet in old age and its implications for interventions
Manuela Zambianchi2
Abstract
Adopting a modified model of Planned Behavior Theory, the study analyzed the role exerted by past adherence to the Mediterranean diet, the belief that the Mediterranean diet can contribute to health in old age, and proactive coping strategies on the intention to improve adherence to the Mediterranean diet in old age. 121 elderly people (Mean age = 68.60; SD = 7.1; 63 males and 51 females, 7 missed this demographic data) took part in the study, using the following instruments: Questionnaire on adherence to the Mediterranean diet (Panagiotakos, Pitsavos, & Stefanidis, 2007); Proactive Coping Inventory (Greenglass, 2002). A single item assessed the belief about the Mediterranean diet being a healthy nutrition model for healthy aging and a single item evaluated intention to improve adherence to the Mediterranean diet. Females prove to be more willing to adhere to the Mediterranean diet, and a higher level of schooling favors its adherence. A General Linear Model highlighted the positive contribution of three independent variables: proactive coping strategies, the belief that the Mediterranean diet helps the elderly to age in good health, and past adherence to this dietary pattern, together with gender, level of education and the interaction between gender and level of education.
Keywords
Mediterranean diet, healthy aging, proactive coping, Planned Behavior Theory.
Introduction
Positive aging: the convergence of high physical performance, high cognitive efficiency and social engagement
The substantial and structural demographic change that is occurring in developed societies highlights the progressive increasing of life expectancy (EUROSTAT, 2019; ISTAT, 2019). This growing relevance of the aging population posits a pressing need for the comprehension of the mechanisms, the processes, and the resources that lead people to a positive aging. The contemporary theoretical perspectives on positive aging have adopted a systemic approach, arguing that this condition requires the presence of high overall level of functioning that is achieved through the possession of physical, personal and social resources. The systemic model of successful aging elaborated by Rowe and Khan (1987, 1997) makes a preliminary distinction between usual aging (marked by a modest decline in several functions, e.g., memory) and successful aging (marked by low risk of diseases and high global functioning). Rowe and Khan define successful aging as a condition that is characterized by the presence of three factors: 1) low probability of diseases and disability; 2) high level of physical and cognitive capacity; 3) active involvement in social life. The presence of high physical resources is strongly related to the involvement in healthy behaviors, such as regular physical activity and the adoption of a healthy dietary pattern, as highlighted the Mc Arthur Study on Successful Aging (Glass et al., 2005).
The Complex Model of successful aging based on Proactive Adaptation, elaborated by Kahana and Kahana (1996), Kahana, Kahana and Zjiang (2005), Kahana, Kelley-More and Kahana (2012), adopts a longitudinal and processual perspective within a multidimensional and multifactorial frame for explaining the different outcomes of the individuals when they reach old age. They adopt an agentic conception of the individual across lifespan arguing that individuals are substantially agentic and proactive across the entire life span, reaching a successful aging through the active use of two fundamental strategies, namely the preventive proactivity and the corrective proactivity. The former refers to strategies and resources aimed at preventing the onset of undesirable outcome (e.g., frailty, age-related diseases, loneliness), while the corrective proactivity refers to strategies and resources aimed at reducing the impact of critical situations or stressors already occurred (e.g., the presence of a chronic diseases, the loss of a loved one). The proactive behaviors aimed at preventing the onset of negative outcomes can be seen as an important new feature in the literature on successful aging, since they concur to preserve those resources that are fundamental for successful aging. Among these proactive behaviors, the proactive coping strategies have become to be regarded as promising area of inquiry for enhancing positive aging (Aspinwall, 2005; Ouweand, De Ridder, & Bensing, 2007; 2008; Thoolen, De Ridder, Bensing, Gorter, & Rutten, 2009; Zambianchi, 2013).
The research on coping strategies until now has mostly focused on those strategies that are set in motion when stressful events have already happened or are happening (e.g., problem solving, emotion management, avoidance, seeking social support). Indeed, coping has been defined as constantly changing cognitive and behavioral efforts to manage specific internal or external demands (Lazarus & Folkman, 1984). Proactive coping is instead directed at stressful events that may occur in the future and for this reason it may be viewed as an active and purposeful coping approach that could be relevant in all areas of life, including health practices promotion and prevention of diseases. There are two major definitions of proactive coping. The former was elaborated by Aspinwall and Taylor (1997) and refers to proactive coping as a set of strategies aimed to prepare individuals for threatening events or to minimize the severity of these events before they happen. The latter was developed by Schwarzer and Taubert (2002) and defines proactive coping as the individual efforts to build up resources that facilitate the personal growth, the achievements of challenging goals and projects in life and the actualisation of talents and potentials. According to this definition, proactive individuals intentionally start constructive paths of action, aimed at modifying the environment, identifying the resources for their development. Both definitions of proactive coping strategies capture a common underlie, the «forward-thinking style» centred on future planning, that individuals utilize to enhance, accumulate or conserve resources that help them to realize desires or projects and to reduce stress and illness, as sustained by the Resources Conservation Theory (Hobfoll, 2003). For this reason, they could be both fundamental for the adoption of healthy behaviors, such as adherence to a healthy dietary pattern that help individuals to avoid or delay frailty, disability or diseases in old age. Several studies have tested the role of proactive coping strategies for the adoption of healthier lifestyles.
Thoolen and collegues (2008) evaluated the efficacy of a proactive self-management course for patients with type 2 diabetes, based on the improvement of proactive coping skills. This intervention was effective in helping patients in dealing with the disease, also improving their goal achievement. A second intervention aimed at achieving improvements in healthy behaviors (diet and physical activity) in diabetes patients (Thoolen et al., 2009) confirmed that proactive coping was a better predictor of long-term self- management compared to self-efficacy. Vinkers, Adriaanse, Kroese and De Ridder (2014), have investigated the role of a pre-treatment based on proactive coping skills on successful weight management in a sample of Dutch adults, confirming that these future-oriented skills are relevant for success in weight management and weight loss maintenance. These results clearly highlight the relevance of this set of future-oriented skills for healthy behaviors in old age.
The Mediterranean diet: a relevant protective nutrition pattern against functional declines in old age
An increasing body of studies have suggested that the adoption of the Mediterranean diet has a significant impact on how well people age.
This type of diet, usually consumed among the population of the Mediterranean Sea since a long time, has been reported to be a whole model of healthy eating and is characterized by a high intake of vegetables, legumes, fruits (typical daily dessert) and nuts, unrefined cereals, a high intake of olive oil as the principal source of fat, a moderately high intake of fish, a low to moderate intake of cheese and yogurt and a low intake of meat (especially red meat, to which the white meat consumption is preferable), zero to four eggs consumed weekly and a regular but moderate consume of red wine, essentially at meals (Tricopolou & Lagiou, 1997). Lasheras, Fernàndez and Patterson (2000), in a study conducted on Italian and Greek elderly people aimed at evaluating the effectiveness of the Mediterranean diet on survival, have shown that this diet appears to be effective, especially in the third age. Knoops and collegues (2004), in the HALE (Longitudinal Study in Europe) Project have investigated the association of individual lifestyle factors (such as moderate alcohol use, physical activity and nonsmoking) and Mediterranean diet on mortality in a ten years longitudinal study on elderly population. High adherence to Mediterranean diet results associated with lower mortality rates from all causes included in the study among individuals aged 70 to 90 years.
Sofi and collegues (2008, 2011) also evidenced the important role exerted by the adoption of the Mediterranean diet in preventing age-related diseases such as diabetes, cardiovascular problems, cancer, neurodegenerative diseases. Trichopoulou, Costacou, Barmia and Tricopolou (2003) have conducted a population-based prospective investigation, highlighting that the adherence to Mediterranean diet is associated with a significant reduction in mortality.
Considering these unequivocal results, the adoption and maintenance of the Mediterranean dietary pattern constitutes a fundamental priority for health promotion in old age, that require investigation about the psychological and psychosocial factors that can favor its accomplishment and maintenance.
Despite these evidences, very few studies have nowadays investigated the role of psychological and psychosocial factors that can improve the adherence to Mediterranean diet as specific whole nutritional model. Several studies indeed have already investigated the role of healthy nutrition (e.g., high consume of fruit and vegetables, see Steptoe et al., 2003; Koethe & Mullan, 2012) on healthy aging, but very few studies have taken into account the Mediterranean diet as a whole.
Sanchez-Villegas and collegues (2002) in a prospective study have identified female gender and high level of school education as structural variables associated with a higher adherence to the Mediterranean dietary pattern. Bonaccio and collegues (2012) have investigated the role of demographic variables such as education and income on adherence to Mediterranean diet in Central Italy (MOLI-SANI Study); they also highlighted that a high income and a better school education were associated with a higher adherence to this nutrition model.
The promotion of a healthy lifestyle. Evidences from the Theory of Planned Behavior
Several models have been used over the past decades to gain a better understanding of the antecedents of engaging in healthy behaviors. The Theory of Planned Behavior (Ajzen, 1991) is one of the major predictive models used in this area of investigation. This model suggests that the proximal determinant of behavior is one’s intention to engage in that behavior, with intentions being determined by three constructs: attitudes (the beliefs about the behaviors and the evaluation of the relevance of the outcome, e.g. the belief that Mediterranean diet is effective in helping people to reach a better physical health, together with the positive evaluation of possessing a good health condition); subjective norms (the social pressure exerted by groups to which the individual belongs on a specific behavior and the desire to accomplish to them), and perceived behavioral control, that refers to the amount of control individuals believe they have over performing a behavior, closely related to the concept of self-efficacy (Bandura, 1997). The Theory of Planned Behavior has been successful in predicting a wide range of health-related behaviors such as smoking cessation, physical activity, adoption of a low-fat diet (Armitage & Conner, 2001). Past behavior is often included as an additional predictor of intentions and behavior within it (Armitage & Conner, 2001). Several authors have examined the efficacy of a modify model of Planned Behavior Theory in predicting healthy dieting behavior. Brouwer and Mosack (2014) have conducted a research with an expanding model of Planned Behavior Theory that included identity (in this case, the healthy eater identity) for predicting a healthy eating in a sample of adult women. They highlight that this new construct was a significant predictor of healthy eating intentions. Koethe, Mullam and Butow (2012) tested the efficacy of Planned Behavior Theory for the promotion of a higher consumption of fruit and vegetables. They found that a program based on emails messages designed on the core assumptions of Planned Behavior Theory (attitudes, subjective norms and behavioral control) increases the consumption of these two nutritional components.
In accordance with the general core assumption of the Planned Behavior Model (the relevance of intentions as the most proximal factor to concrete behavior, and of the beliefs about the behavior that have to be performed), and in lights of the findings on proactive coping strategies for healthy nutrition in old age, our study has focused on a modified model of Planned Behavior Theory, which evaluated the predictive power of proactive coping strategies — in the conceptualization of Aspinwall and Taylor (1997) and Schwarzer and Taubert (2002)—, past behavior (defined by the monthly level of adherence to a Mediterranean nutrition style) and the belief about the relevance of Mediterranean diet as healthy dietary style on the intention to improve the adherence to the Mediterranean diet in the near future. Having several researches demonstrated that the subjective norms give a small contribution to the explained variance for behavioral intentions (Godin & Kok, 1996), this component of the Planned Behavior model were not included in our research.
Aims and hypotheses
The study had the following four aims and tested the following hypotheses.
- H1. To examine the level of past adherence to Mediterranean diet, the belief about its effectiveness for health in old age, and the level of utilization of the proactive coping strategies by the elderly.
- H2. To examine the differences for gender and level of education on proactive coping strategies, Mediterranean diet past consume, the belief about its efficacy in promoting health and the intention to improve its adherence. It was hypothesized, basing on previous literature (e.g. Sanchez-Villegas et al., 2002; Bonaccio et al., 2012), that females are more compliant to this dietary pattern than males, and that those with a high educational level are more willing to change their dietary lifestyle or improve their adherence to Mediterranean diet.
- H3. To examine the correlations among proactive coping strategies, Mediterranean diet past adherence, the belief about its health promotion and the intention to improve its adherence. It was hypothesized positive correlations between the intention to improve its adherence, the belief about its efficacy, the proactive coping strategies and the past adherence to Mediterranean diet.
- H4. To evaluate the contribution of the proactive coping strategies, past Mediterranean diet adherence, and the belief about Mediterranean diet on the intention to improve its adherence in the near future, after controlling for gender, level of education and the interaction between gender and level of education. Age was inserted as continuous variable. It was hypothesized that the proactive coping strategies, the past adherence to Mediterranean diet, the belief that it can help old people in improving health give a positive contribution to the explained variance for the intention to improve the adherence to Mediterranean diet in the near future.
Method
Participants
The study involved a sample of 121 old people (M = 68.60; S.D. = 7.1), 63 males and 51 females; 7 missed this data. For school education, 1% does not possess any level of school education, 11% possess the Elementary School License, 26% possess the Middle School Diploma, 41 % possess the High School Diploma and 20% a University Degree.
Measures
After giving their consent, the participants filled in, in about half an hour, the following self-report measures.
Questionnaire on Proactive Coping (P.C.I.) (Greenglass et al., 2002; Comunian, Grrenglass and Schwarzer, 2003). This consists of 7 scales; we selected three scales: proactive coping (14 items, with α = 0.87) that assesses the attitude toward striving for a better future (e.g. of item: ‘‘After attaining a goal, I look for another, more challenging one’’), reflective coping (11 items, with α = 0.77), that assesses the ability to visualize future scenarios (e.g. of item: ‘‘I think about every possible outcome to a problem before tackling it’’) and preventive coping (10 items, with α = 0.77) that assesses the processes through which one prepares for potential future stressors (e.g. of item: ‘‘I make plans of things to do before bad events happens’’), with a score ranging from 1 (not at all true) to 4 (completely true). These scales were chosen because they represent the fundamental forward-looking sub-scales (preventive and reflective coping) and resource-based sub-scale (proactive coping) highlighted by Schwarzer and Taubert (2002).
Questionnaire on Adherence to Mediterranean diet (Panagiotakos et al., 2007). It evaluates the monthly consumption of the following food groups: non-refined cereals (whole grain bread and pasta, brown rice, etc), fruit, vegetables, legumes, potatoes, fish, meat and meat products, poultry, full fat dairy products (like cheese, yoghurt, milk), as well as olive oil. In particular, individuals rating was assigned from 0 = «never» to 5 = «more than 18 times in one month». Potatoes, although they are not in the basis of the Mediterranean pyramid, were included in this group of foods since they are a good source of vitamins C, B1 and B2, niacin, carbohydrates, fiber, potassium and magnesium, which have been associated with cardiovascular disease risk markers in previous studies (Friedman, 2004, in Panagiotakos et al., 2007). Having a medium-low score on dietary products, a low score on red met and high scores on the other items is indicative of adherence to Mediterranean diet. Factor analysis has shown a two-factor solution, with the first factor gathering five items (cereals, vegetables, fruit, olive oil, legumes) with α = 0.71, and the second factor gathering four items (red meat, white meat, milk/cheese, potatoes) with unsatisfactory scale reliability (α = 0.50). The subsequent analyses were than conducted only on the first factor, that represents the «core» elements of Mediterranean diet (Sànchez-Villegas et al., 2002). The consumption of fish did not enter in any factors, due to its low loading (<0.40).
A single item assessed the intention to adhere more to Mediterranean diet in the future (with a five-point Likert scale: 1 = «not at all»; 5 = «completely true»).
A single item assessed the belief that Mediterranean diet can help old people in reaching a healthy aging (with a five-point Likert scale: 1= «completely disagree»; 5 = «completely agree»).
Procedures
The participants were recruited at Senior Centers, Popular University, Trade Unions for retired, Cultural Centers and recreational organizations in North Italy (Romagna). They were contacted by the direction of their respective Institutions. The participants who voluntary agreed to participate were informed about the anonymity of the questionnaire and briefly about the principal aims of the research.
Statistical analyses
Statistical analyses were run in four steps. Firstly, means, standard deviations, skewness and kurtosis were calculated for all variables. In the second step, Manova models were run in order to assess the influence of socio-demographic variables (gender and level of education) on proactive coping strategies, past adherence to Mediterranean diet, the belief about its healthy function and the intention to improve it in the future. Age was inserted as continuous variable. Univariate analyses of variance (ANOVA) were subsequently run in order to identify the structural variables that have shown significant different scores among sub-groups. In the third step, a correlational matrix (Spearman correlation, due to the not Gaussian shape of the variable «monthly past consume of Mediterranean diet») was calculated. In the fourth step, a General Linear Model (GLM) was run for evaluating the contribution to the intention to improve the adherence to Mediterranean diet, since through GLM it is possible to evaluate a whole model that comprises also the interaction of categorical variables on the dependent variable.
Results
Descriptive of study variables
The monthly consume of cereals, fruit, vegetables and olive oil is high (M = 5.70; S.D = 0.85), while it is evidenced a low intake of poultry, fish and legumes (see table 1).
For the three proactive coping strategies, preventive coping strategies are the most utilized (M = 3.15; S.D. = 0.46), while the proactive coping strategies are the less utilized (M = 2.97; S.D = 0.54). The monthly adherence to overall Mediterranean diet pattern is high (M =5.05; S.D. = 0.76) (see table 2).
The belief that adhering to Mediterranean diet can favor a healthy aging shows a high score (M = 4.47; SD = 0.68) (see table 2).
Differences for gender and educational level on study variables
A Manova model highlights differences between males and females for proactive coping strategies that approaches significance (Wilk’s lambda = 0.93; F (3,110) = 2.4; p <0.07). Subsequent Univariate Anova highlights that males utilize significantly more often than females the preventive coping (F = 5.91; p<0.01; Males M = 3.24; SD = 0.40; Females M = 3.03; SD = 0.52; Scheffè post hoc test: p<0.01).
Females are more willing to improve their adherence to Mediterranean diet than males (F = 3.89; p<0.05; Females M = 4.19, SD = 0.77; Males M = 3.94, SD = 1.0; Scheffè post hoc test: p <0.05).
The level of school education influences the belief about Mediterranean diet as promotional factor of healthy aging (F = 3.7; p<0.01): old people with a higher educational level believe more strongly that this diet can help them to reach a healthy aging than those with lesser school education (Elementary License M = 3.38, S.D. = 1.26; Middle School License M = 4.00, S.D. = 0.84; High School Diploma M = 4.12, S.D. = 0.89; University Degree M = 4.12, S.D. = 1.0; Tukey post hoc test: significant for groups 1-2 and for groups 2-3-4 (no statistical significance between groups 2-3).
Correlations among study variables
The intention to improve the adherence to Mediterranean diet is positively correlated with the belief that it could help old people to reach a healthy aging, with the monthly past adherence to it and with the proactive coping strategies (active investment in resources and growth) (see table 3).
Table 1
Descriptive values of Mediterranean diet adherence (monthly consumption of specific foods)
|
M |
DS |
Skewness |
Kurtosis |
|
|
Cereals (pasta, rice) |
5.11 |
1.34 |
-1.42 |
0.79 |
|
Potatoes |
2.97 |
1.04 |
0.73 |
0.40 |
|
Fruit |
5.54 |
1.04 |
-2.55 |
6.0 |
|
Vegetables |
5.45 |
1.11 |
-2.07 |
3.21 |
|
Legumes |
3.49 |
1.25 |
0.34 |
-0.53 |
|
Fish |
3.40 |
1.25 |
0.38 |
-0.52 |
|
Red meat |
3.42 |
1.26 |
0.18 |
-0.64 |
|
Poultry |
3.26 |
1.13 |
0.43 |
0.32 |
|
Diary |
4.21 |
1.52 |
-0.20 |
-1.3 |
|
Olive oil |
5.70 |
0.85 |
-3.13 |
9.3 |
Table 2
Descriptive values of study variables
|
M |
DS |
Skewness |
Kurtosis |
|
|
Belief that Med. diet help old people |
4.47 |
0.69 |
-0.99 |
-0.27 |
|
Intention to improve adherence to Med. diet |
4.02 |
0.95 |
-0.93 |
0.86 |
|
Monthly past adherence to Medit.diet.* |
5.05 |
0.76 |
-1.99 |
4.55 |
|
Proactive coping |
2.97 |
0.54 |
-0.50 |
0.76 |
|
Preventive coping |
3.15 |
0.46 |
-0.79 |
0.94 |
|
Reflective coping |
3.10 |
0.48 |
-0.49 |
0.16 |
|
*(cereals, vegetables, fruit, olive oil, legumes) |
*Only the factor with these dietary products was computed here N= 121
Table 3
Correlations among study variables
|
Variables |
1 |
2 |
3 |
4 |
5 |
6 |
|
1. Intention to improve the adherence to M. diet |
- |
|||||
|
2. Belief about M. diet |
0.44*** |
--- |
||||
|
3. Past adherence to M. diet |
0.23*** |
0.24** |
--- |
|||
|
4. Proactive coping |
0.24** |
0.14 |
0.14 |
--- |
||
|
5. Preventive coping |
0.08 |
0.05 |
0.16+ |
0.68*** |
-- |
|
|
6. Reflective coping |
0.09 |
0.10 |
0.13 |
0.73*** |
0.78*** |
--- |
+ = p<0.08; ** = p<0.01; *** = p<0.001 N= 121
The contributors to the intention to improve the adherence to Mediterranean diet in the near future
A General Linear Model with the intention to improve the adherence to Mediterranean diet as dependent variable was performed. The belief about the healthy value of Mediterranean diet for old people, the three proactive coping strategies and the past adherence to Mediterranean diet entered as independent variables, together with age, gender, level of education and the interaction between gender and level of education. Age was inserted as continuous variable. In the first step, structural variables (age, gender, level of school education) entered into the equation, giving a 7% of contribution for the explained variance of the model (adj. R2= 0.07; p<0.05). Gender and school education, together with the interaction between gender and school education resulted as significant.
In the second step entered into the model the belief about Mediterranean diet, the past consume of it and the three proactive coping strategies.
The intention to improve the adherence to the Mediterranean diet was significantly associated to the belief on its efficacy, the past adherence to it, the proactive coping strategies conceptualized as active engagement in life, growth and actualization of potentials (Schwarzer & Taubert, 2002), gender, level of education and the interaction between gender and education. For this latter factor, males with low school education possess the lowest score on intention to adhere in the future to the Mediterranean diet, while females with the equal school level present a higher score on it (Multiple R = 0.63; R2 = 0.40; adj. R2 = 0.31; F (13, 95) = 4.89; p<0.001) (see table 4 and figure 1).
Table 4
General Linear Model. Intention to improve the adherence to Mediterranean diet as dependent variable. (Multiple R = 0.63; R2 = 0.40; adj. R2 = 0.31; F (13, 95) = 4.89; p<0.001)
|
Independent variables |
Beta |
st. error of Beta |
|
Belief that med. Diet help old people |
0.35*** |
0.09 |
|
Past adherence to Mediterranean diet |
0.27** |
0.08 |
|
Proactive coping |
0.34** |
0.13 |
|
Preventive coping |
-0.10 |
0.15 |
|
Reflective coping |
-0.18 |
0.16 |
|
Gender |
-0.28** |
0.09 |
|
Level of education |
-0.29** |
0.09 |
|
Gender* level of education |
-0.31** |
0.10 |
|
Age |
0.05 |
0.06 |
**p<0.01;***p<0.001 N = 112
Figure 1
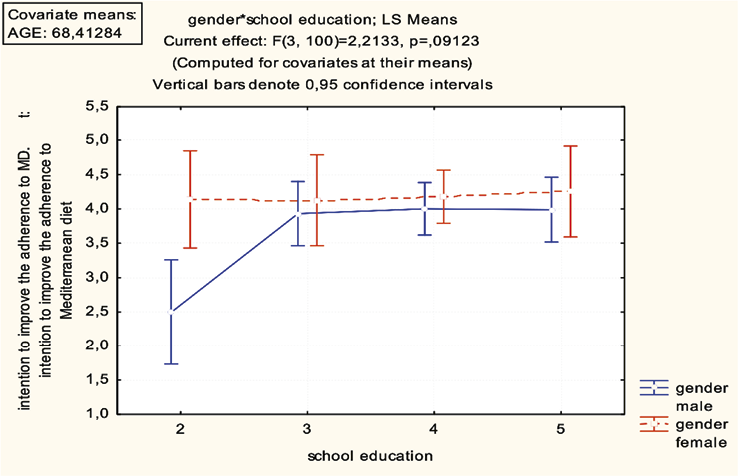
Interaction between gender and level of school education for the intention to improve the adherence to Mediterranean diet
Discussion and Conclusions
Adopting a modified model of the Planned Behavior Theory (Ajzen, 1991), the study has analyzed the relevance of proactive coping strategies, the belief about Mediterranean diet as a pattern of healthy nutrition for healthy aging and past monthly consume of Mediterranean intake on the intention to improve the adherence to this healthy nutrition pattern in a sample of old people.
The old people show a high consume of olive oil, cereals, fruit and vegetables, that are among the most important components of Mediterranean diet (Tricopolou, 2003). At the same time, however, their consume of fish and legumes is not particularly high, despite their fundamental protective functions (Angeloni, Giusti, & Hrelia, 2019; Malaguti et al., 2014; Sofi et al., 2008). The high consume of Mediterranean typical foods, such as cereals, fruit, vegetables, olive oil in this group of elderly could be explained through the belonging of Italy to Mediterranean culture, where this dietary model is widespread (Tricopolou & Lagiou, 1997). The elderly also believe that Mediterranean diet can help old people in reaching a healthy aging, as evidenced by the high score reported on this item.
Referring to socio-demographic factors, this study confirms the relevance of educational school level for a higher adherence to Mediterranean food consumption. The old people that possess a high level of school education are more willing to modify their nutrition style. The study also confirms the existence of gender differences, as already highlighted by Sànchez-Villegas and collegues (2002) and Zambianchi (2016). Females are more willing to change their dietary pattern in favor to Mediterranean diet in the future than males, especially if males do not possess high cultural resources, as highlighted the results of General Linear Model. Those elderly that show the lowest level of adherence to Mediterranean dietary pattern are indeed males with Elementary school License, while females with the same low school attainment present a higher adherence to it. Possessing the Mediterranean diet a protective function against diseases and mortality, its importance can be perhaps better evaluated and appreciated by those who have high cultural resources and hence are able to understand the mechanisms and the processes that operate at biological level, and are more willing to improve their cultural competencies in health issues. At the same time, the higher score of females (independently from their educational school attainment) could be related to the different educational models for gender, when, at least several decades ago, females were encouraged to take care of the house and the meals. This role could have made old women more sensitive to the question of healthy eating.
The results highlight that the belief about Mediterranean diet and the past adherence to it are positively associated with the intention to improve this nutrition model, confirming the basic assumption of the Planned Behavior Theory about the role exerted by our past behavior and the relevance of the beliefs. Perhaps, having a well-established healthy lifestyle can make people to appreciate its efficacy in promoting health, especially in old age (Sofi et al., 2010). Among the three proactive coping strategies, those related to active intervention in the lifer context and the search for self-realization and growth appear to be positively associated to the intention to adhere more to Mediterranean diet. These results were also strengthened through the General Linear Model. The proactive coping strategies in the conceptualization of Schwarzer and Taubert (2002) positively are associated to the intention to improve the adherence to Mediterranean diet. Having life projects, believing that our actions can modify the context of life or believing that new experiences or novelty have to be seen as challenges and not as threat, (that is the core conception of proactivity and human agency, see Bandura, 1997; Elder jr., 1994), perhaps may constitute a promotional resource for healthy aging and may be regarded as motivational force for safeguarding the health status through the adoption and maintenance of a healthy lifestyle.
Contrary to our hypothesis, the preventive and reflective coping strategies are not contributors of the improvement of Mediterranean diet adherence. Our study has not taken into account old people with specific dietary problems, such as diabetes or obesity, as previous research on proactive skills (e.g., Thoolen et al. 2009). For this reason, the issue of disease prevention seems to be not central; the Mediterranean dietary whole model can be perceived as «general healthy nutrition style» and not associated with a future perspective of disease prevention. It may be that preventive and reflective coping strategies are set in motion when nutrition is placed in a clear perspective of prevention of diseases such as diabetes. Future studies could better clarify this crucial point, relevant for health education of the elderly.
Age did not influence the willingness to improve the adherence to the Mediterranean diet, contrary to results obtained by Sànchez -Villegas and collegues (2002), where it was found an increase in adherence from youth to old age. It may be because our study did not take into account previous life-stage, but only old age from the third age to the fourth age (octogenarians) and is based on a small sample size.
Limits of the study
This study has several important limits, that have to be taken into account. As already pointed out, the small sample of old people do not permit the extension of our results to the old Italian population. Future studies, with broader samples are necessary in order to confirm the results here presented. The use of a single item to assess the belief about Mediterranean diet also constitutes a serious limit to the study, together with the high number of variables tested on a small sample of old people.
Potentials and future research’s avenues.
Studies that will take into account the complete Planned Behavior Model, including the subjective norms and the perceived control over the healthy behavior could provide for a better explanation of the strengths and potentials of this model for the adoption of this healthy diet in old age. The relevance of proactive coping strategies as resources accumulation, actualization of potentials and agentic management of life context confirms the research of Kahana and collegues (2013) and might open a new promising area of research and intervention for the promotion of a healthy lifestyle in old age (Ouweand et al., 2007; Thoolen et al., 2009; Zambianchi, 2013).
Future research’s lines might further examine the effectiveness of interventions (e.g., training programs) targeted on old population and aimed at modifying the unhealthy dietary styles and promoting a more adherence to the Mediterranean diet based on the components of the Planned Behavior Model.
References
Ajzen, I. (1991). The Theory of Planned Behavior. Organizational Behavior and Human Decision Processes, 50, 179-211.
Angeloni, C., Giusti, L., & Hrelia, S. (2019). New neuroprotective perspectives in fighting oxidative stress and improving cellular energy metabolism by oleocanthal. Neural Regeneration Research, 14 (7), 1217-1218. https://doi.org/10.4103/1673-5374.251327
Armitage, C.J., & Conner, M. (2001). Efficacy of the theory of planned behavior. A meta- analytic review. British Journal of Social Psychology, 40, 471-499.
Aspinwall, L. G., & Taylor, S.E. (1997). A stitch in time: self-regulation and proactive coping. Psychological Bulletin, 121, 417-436.
Aspinwall, L. (2005). the Psychology of Future-Oriented Thinking: From Achievement to Proactive Coping, Adaptation, and Aging. Motivation and Emotion, 29(4), 203-235, doi: 10.1007/s11031-006-9013-1
Bandura, A. (1997) Self-efficacy: the exercise of control. New York: Freeman.
Bonaccio, M., Bonanni, A. E., Castelnuovo, A., De Lucia, F., Donati, M. B., De Gaetano, G., & Iacoviello, L. (2012). Low income is associated with poor adherence to Mediterranean diet and a higher prevalence of obesity: cross-sectional results from the Moli-sani study. British Medical Journal, 2, 1-9. doi:10.1136/bmjopen-2012-001685
Bouwer, A., & Mosack, K.E. (2014). Expanding the theory of planned behavior to predict healthy eating behaviors. Exploring a healthy eater identity. Nutrition & Food Science, 1, 39-53.
Comunian, L., Greenglass, E. R., & Schwarzer, R. (2003). The proactive coping inventory-Ital- ian version. Retrived November 27, 2020, from http://userpage.fu-berlin.de/~health/ital_pci.htm
Engel, G. L. (1977). The Need for a New Medical Model: A Challenge for Biomedicine. Science, 196, 4286,129-36.
EUROSTAT (2019). Population structure and ageing. Retrieved November 27, 2020, from https://ec.europa.eu/eurostat/statistics-explained/index.php/Population_structure_and_ageing
Flick, U. (1998). The social construction of individual and public health: contributions of social representations theory to a social science. Social Science Information, 37, 639-662.
Flick, U., Fisher, C., Neuber, A., Friedrich, W.S., & Walter, U. (2003). Health in the context of growing old: social representation of health, Journal of Health Psychology, 8, 539-556.
Friedman, M. (2004). Analysis of biologically active compounds in potatoes (Solanum tuberosum), tomatoes (Lycopersicon esculentum), and jimson weed (Datura stramonium) seeds. Journal of Chromatography A, 1054(1-2), 143-145.
Glass, T.A., Seeman, T.E., Herzogh, A.R., Kahn, R., & Berkman, L. F. (1995). Change in productive activity in late adulthood: Mac Arthur Studies of Successful Aging. Journal of Gerontology: Social Science, 50B(2), S65-S76.
Godin, G., & Kok, G. (1996). The theory of planned behaviour: A review of its applications to health-related behaviours. American Journal of Health Promotion, 11, 87-98.
Greenglass, E. R. (2002). Proactive coping and quality of life management. In E. Frydenberg (Ed.), Beyond coping: Meeting goals, visions, and challenges (pp. 37-62). Oxford, England: Oxford University Press.
Hobfoll, S.E. (2003). The influence of culture, community and the nested self in the stress process. Advancing conservation of resources theory. Applied Psychology: An International Review, 3, 337-370. doi: 10.1111/j.2044-8325.2010.02016.x
Kahana, E., Kahana, B., & Zjiang, J. (2005). Motivational antecedents of preventive proactivity in late life: Linking future orientation and exercise. Motivation and Emotion, 29, 443-464.
Kahana, E., & Kahana, B. (1996). Conceptual and empirical advances in understanding aging well through proactive adaptation. In V. Bengtson (Ed.) Adulthood and aging: Research on continuities and discontinuities (pp. 18-41). New York: Springer Publishing.
Kahana, E., Kelley-Moore, J., & Kahana, B. (2012). Proactive aging: a longitudinal study of stress, resources, agency and well-being in late life. Aging & Mental Health, 4, 438-451.
Knoops, K.T.B., de Groot, L.C.P., Kromhout, D., Perrin, A.E., Moreiras-Varela, O., Menotti, A., van Staveren, W.A. (2004). Mediterranean Diet, lifestyle factors, and 10-year mortality in elderly European men and women. Journal of American Medical Association (JAMA), 22, 1433-1439.
Kothe, E.J., Mullan, B.A., & Butow, P. (2012). Promoting fruit and vegetable consumption. Testing an intervention based on the theory of planned behavior. Appetite, 3, 997-1004.
Lasheras, C., Fernández, S., & Patterson, A.M. (2002). Mediterranean Diet and Age with Respect to Overall Survival in Institutionalized, Nonsmoking Elderly People. American. Journal of Clinical Nutrition, 71, 987-992.
Lazarus, R., & Folkman, S. (1984). Stress, appraisal and Coping. New York: Springer.
Malaguti, M., Dinelli G., Leoncini E., Bregola V., Bosi S., Cicero, A.F.G., & Hrelia, S. (2014). Bioactive peptides in cereals and legumes: Agronomical, Biochemical and Clinical Aspects. International Journal of Molecular Sciences, 15, 21120-21135.
Ouwehand, C., De Ridder, D.T.D., & Bensing, J. (2007). A Review of successful aging models: Proposing proactive coping as an important additional strategy. Clinical Psychology Review, 27(8), 873-884.
Ouwehand, C., De Ridder, D.T.D., & Bensing, J. (2008). Individual differences in the use of proactive coping strategies by middle-aged and older adults. Personality and Individual Differences, 45, 28-33.
Panagiotakos, D., Pitsavos, C., & Stefanidis, C. (2007). Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the Mediterranean Diet Score. Preventive Medicine, 4, 335-340. doi: 10.1016/j.ypmed.2006.12.009
Rowe, J.W., & Khan, R.L. (1987). Human aging: Usual and successful. Science, 237(4811), 143-149.
Rowe, J.W., & Khan, R.L. (1997). Successful aging. The Gerontologist, 37, 433−440.
Sanchez-Villegas, A., Martinez, J.A., De Irala, J., Martinez-Gonzales, M.A., and members of the SUN research group (2002). Determinants of the adherence to an “a priori» defined Mediterranean dietary pattern. European Journal of Nutrition, 41, 249-257
Schwarzer, R., & Taubert, S. (2002). Tenacious goal pursuits and striving toward personal growth: proactive coping. In E. Fydenberg (Ed.), Beyond coping: Meeting goals, visions and challenges (pp. 19-35). London: Oxford University Press.
Sofi, F., Abbate, R., Gensini, G.F., & Casini, A. (2010). Accruing evidence on benefits of adherence to the Mediterranean diet on health: an updated systematic review and meta-analysis. American Journal of Clinical Nutrition, 2, 1189-1196. doi: 10.3945/ajcn.2010.29673
Sofi, F., Cesari, F., Abbate, R., Gensini, G.F., & Casini, A. (2008). Adherence to Mediterranean Diet and health status: meta-analysis. British Medical Journal, 337, a1344. doi: 10.1136/bmj.a1344
Steptoe, A., Perkins-Porras, L., McKay, C., Rink, E., Hilton, S. & Cappuccio, F. (2003). psychological Factors Associated with Fruit and Vegetables Intake and with Biomarkers in Adults from low-Income Neighborhood. Health Psychology, 22, 2, 148-155. doi: 10.1037/0278-6133.22.2.148
Thoolen, B.J., De Ridder, D., Bensing, J., Gorter, K, & Rutten, G. (2008). Beyond good intentions: the development and evaluation of a proactive self-management course for patients recently diagnosed with type 2 diabetes. Health Education Research, 1, 53-61.
Thoolen, B.J., De Ridder, D., Bensing, J., Gorter, K, & Rutten, G. (2009). Beyond good intentions: the role of proactive coping in achieving sustained behavioural change in the context of diabetes management. Psychology & Health, 3, 237-254.
Trichopolou, A. & Lagiou, P. (1997). Healthy traditional Mediterranean diet: an expression of culture, history and lifestyle. Nutritional Reviews, 11, 383-389.
Tricopolou, A., Costacou, T., Barmia, C., & Trichopolou, D. (2003). Adherence to Mediterranean Diet and survival in a Greek population. The new England Journal of Medicine, 26, 2599-260.
Vinkers, C.D.W., Adriaanse, M.A., Kroese, F.M., & De Ridder, D.T.D. (2014). The role of pre-treatment proactive coping skills in successful weight management. Eating Behaviors, 15, 515-518.
Zambianchi, M. (2013). L’invecchiamento ottimale. Una Rassegna sui principali modelli teorici e sulle strategie proattive in grado di promuoverlo (Optimal aging. A review on principal theoretical models and proactive strategies that promote it). Ricerche di Psicologia, 1, 9-43. doi: 10.3280/RIP2013-01001
Zambianchi, M. (2016). Life Skills Education in età anziana. Un progetto per promuovere il pensiero critico (Life Skills Education in old age. A project for promoting critical thinking). Counseling. Giornale Italiano di Ricerca e Applicazioni, 9(2). doi: 10.14605/CS921615

